|
|
Paget Disease
Osteoporosis Circumscripta
General Considerations
- Multifocal chronic skeletal disease due
to chronic paramyxoviral infection
- Found in about 3% of individuals >40 years; 10% of persons >80 years
- Strong male to female ratio of 2:1
- Histology
- Increased resorption and increased
bone formation
- Newly formed bone abnormally soft
with disorganized trabecular pattern
- Active or Osteolytic phase
- Aggressive bone resorption with lytic
lesions
- Inactive or Quiescent phase
- Decreased bone turnover with skeletal
sclerosis and thickening of the cortex
- Mixed pattern
- Lytic and sclerotic phases frequently
coexist
Clinical Findings
- Most patients are asymptomatic
- When symptomatic, symptoms may include
- Fatigue
- Enlarging hat size
- Peripheral nerve compression
- Neurologic disorders from
compression of brainstem (basilar invagination)
- Hearing loss, blindness
- Facial palsy (narrowing of neural
foramina) - rare
- Pain from the primary disease process
is rare so think of
- Pathologic fracture
- Malignant transformation
- Secondary degenerative joint
disease aggravated by skeletal deformity
- High-output congestive heart failure
from markedly increased perfusion (rare)
- Increased alkaline phosphatase
(increased bone formation)
- Hydroxyproline increased (increased
bone resorption)
- Normal serum calcium and phosphorus
- Sites of involvement
- Pelvis (75%) most common, followed
by
- Lumbar spine
- Thoracic spine
- Proximal femur
- Calvarium
- Scapula
- Distal femur
- Proximal tibia
- Proximal humerus
Imaging Findings
- Imaging Findings
- Classical triad
- Thickening of the cortex
- Accentuation of the trabecular
pattern
- Increased size of bone
- Cyst-like areas
- Skull
- Inner and outer table involved
- Leads to diploic widening
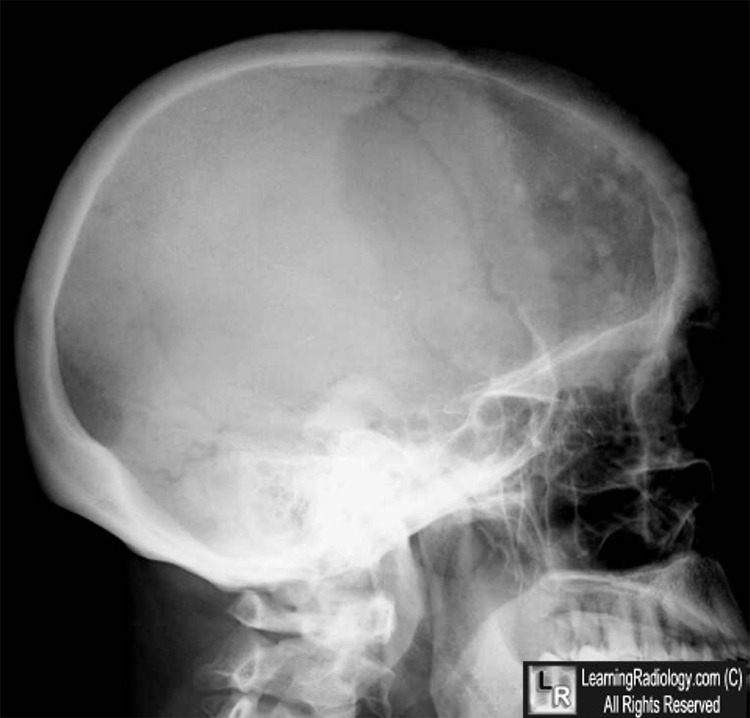
- Osteoporosis circumscripta is
well-defined lysis, most commonly in frontal bone
producing well-defined geographic lytic lesion in skull
- Represents early destructive phase
of disease active stage
- "Cotton wool" appearance represents
mixed lytic and blastic pattern of thickened calvarium (later
stage)
- Basilar invagination with encroachment
on foramen magnum
- Deossification and sclerosis in maxilla
- Sclerosis of skull base
- Long bones (almost invariably starts at
end of bone)
- "Candle flame" or "blade of grass"
pattern of lysis is the advancing tip of V-shaped lytic
defect in diaphysis of long bone originating in subarticular
site
- Lateral curvature of femur
- Anterior curvature of tibia (commonly
resulting in fracture)
- Pelvis
- Thickened trabeculae in sacrum, ilium
- Rarefaction in central portion of
ilium (looks like a large lytic lesion)
- Thickening of iliopectineal line
- Acetabular protrusio with secondary
degenerative joint disease
- Spine (upper cervical, low dorsal,
midlumbar most common sites)
- Coarse trabeculations at periphery of
bone
- "Picture-frame vertebra" mimics
bone-within-bone appearance
- Enlarged vertebral body with
reinforced peripheral trabeculae and more lucent center,
typically in lumbar spine
- "Ivory vertebra" is a blastic vertebra
with increased density
- Ossification of spinal ligaments,
paravertebral soft tissue, disk spaces can occur
- Bone scan
- Sensitivity
- Scintigraphy and radiography (60%)
- Scintigraphy only (27%)
- Radiography only (13%)
- Usually markedly increased uptake
(symptomatic lesions strikingly positive)
- Normal scan may occur in some
burned-out lesions
- Marginal uptake can be seen in lytic
lesion
- MR
- Hypointense area / area of signal void
on T1WI and T2WI (cortical thickening, coarse trabeculation)
- Widening of bone
- Reduction in size and signal intensity
of medullary cavity due to replacement of
high-signal-intensity fatty marrow by medullary bone
formation
- Focal areas of higher signal intensity
than fatty marrow (from cyst-like fat-filled marrow spaces)
- Areas of decreased signal intensity
within marrow on T1WI and increased intensity on T2WI
Complications
- Complications
- Associated neoplasia (0.7-20%)
- Sarcomatous transformation into osteosarcoma (22-90%)
- Fibrosarcoma /malignant fibrous histiocytoma (29-51%)
- Chondrosarcoma (1-15%)
- Sarcomas are usually osteolytic in
pelvis, femur, humerus
- Giant cell tumor occurs in 3-10%
- Lytic expansile lesion in skull,
facial bones
- Lymphoma or plasma cell myeloma are
reported
- Fracture
- "Banana fracture" = tiny horizontal
cortical infractions (“Looser lines”) on convex surfaces
of lower extremity long bones (lateral bowing of femur,
anterior bowing of tibia)
- Compression fractures of vertebrae
- Early-onset osteoarthritis
Treatment
- Treatment
- Calcitonin, diphosphonate, mithramycin
Differential Diagnosis
- Differential diagnosis
- Depends on the bone in which it occurs
- Skull
- Osteolytic or osteoblastic
metastases
- Long bones
- Metastases
- Chronic osteomyelitis (thickened
cortex)
- Old trauma (thickened cortex)
- Hodgkin’s disease
- Spine


Osteoporosis Circumscripta. Top. Lateral skull radiograph shows a large geographic, lytic lesion in the left frontal bone (blue arrows). Also seen are islands of bone (white arrows) producing a "cotton-wool" appearance.
For these same photos without the arrows, click here and here
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}